Multiple studies agree that mask wearing is highly effective, and even moreso in confined spaces/close quarters. In a study done onboard Navy ships it reduced transmission by 70%.
Do these studies replicate the idiotic process of giving everyone a drink so 90% of the people in the confined space take of their mask to snack and drink?
And many studies say the opposite, unfortunately studies are more or less junk. Non-profit research just isn't usefully reliable.
Fortunately we don't really need studies here. A study is an attempt to figure out what would happen if everyone were forced to wear masks, but we did that already. Mask mandates get added, removed and changed at different times even in places that are physically next to each other, allowing us to see what it means in reality - which is nothing. States, counties, cities next to each other that differed only in mask mandates have identical case curves.
If masks actually worked, this data shouldn't be possible. There'd have to be a clear difference in outcomes. For instance this debate doesn't come up with vaccines except in the form "the real world stats appear to show some effectiveness against hospitalization and death, but are they reliable/interprted correctly?". Whereas here there are no real world stats showing effectiveness, only a handful of worthless studies that invariably seem to have major methodological errors when examined.
I'm sure actual gas masks would work, hopefully, but if you come up with a definition of "mask" that nobody actually uses and then claim mask mandates work, or even that masks work, then it's the same as admitting they don't really work.
> There is ample evidence that masking and social distancing are effective in reducing severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission. However, due to the complexity of airborne disease transmission, it is difficult to quantify their effectiveness, especially in the case of one-to-one exposure. Here, we introduce the concept of an upper bound for one-to-one exposure to infectious human respiratory particles and apply it to SARS-CoV-2. To calculate exposure and infection risk, we use a comprehensive database on respiratory particle size distribution; exhalation flow physics; leakage from face masks of various types and fits measured on human subjects; consideration of ambient particle shrinkage due to evaporation; and rehydration, inhalability, and deposition in the susceptible airways. We find, for a typical SARS-CoV-2 viral load and infectious dose, that social distancing alone, even at 3.0 m between two speaking individuals, leads to an upper bound of 90% for risk of infection after a few minutes. If only the susceptible wears a face mask with infectious speaking at a distance of 1.5 m, the upper bound drops very significantly; that is, with a surgical mask, the upper bound reaches 90% after 30 min, and, with an FFP2 mask, it remains at about 20% even after 1 h. When both wear a surgical mask, while the infectious is speaking, the very conservative upper bound remains below 30% after 1 h, but, when both wear a well-fitting FFP2 mask, it is 0.4%. We conclude that wearing appropriate masks in the community provides excellent protection for others and oneself, and makes social distancing less important.
In Germany FFP2/N95/KN95 masks are mandated in many places and situations. Only few people wear them with a tight fit though.
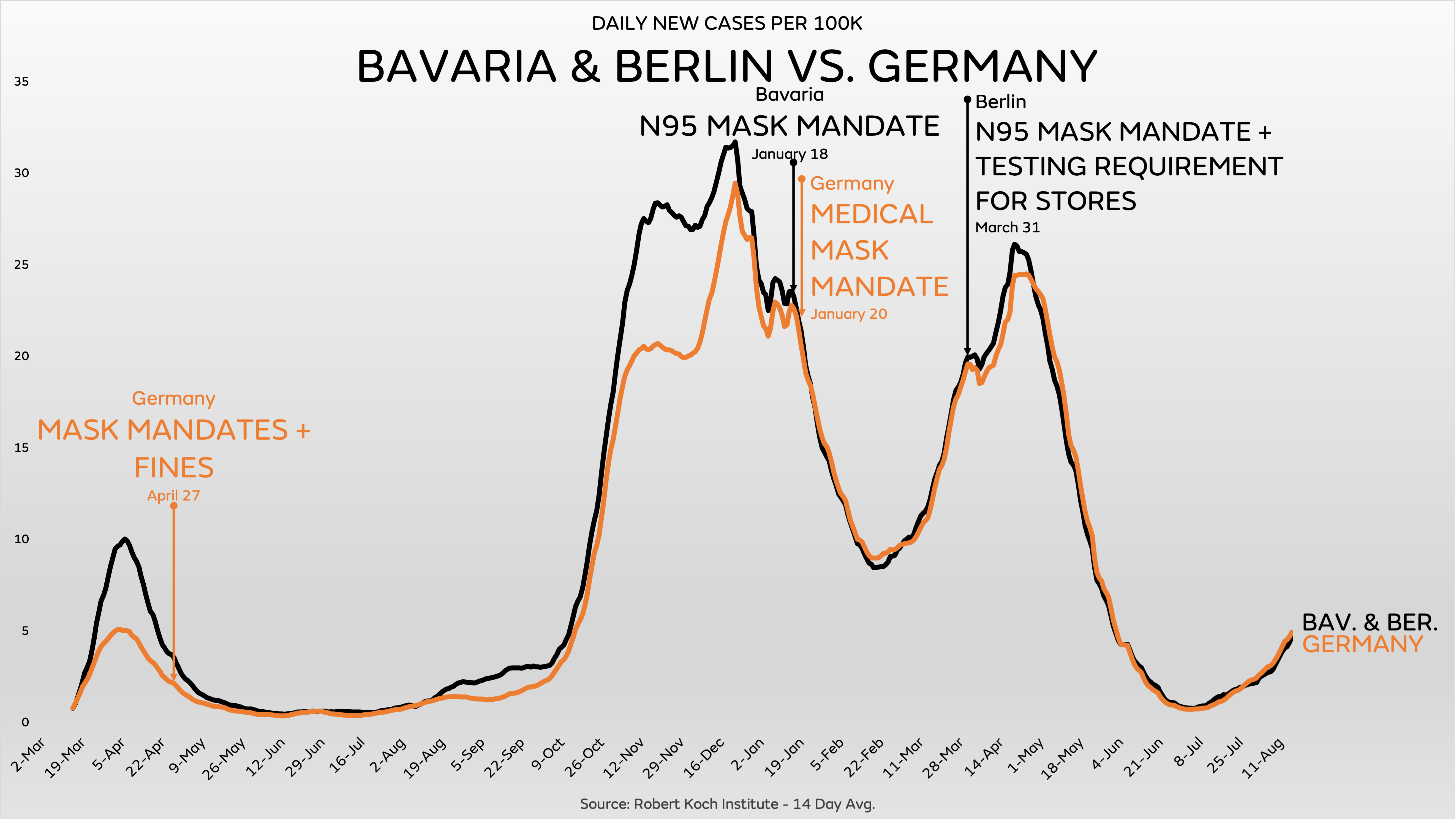
Germany provides a good counterpoint, because some very nearby places differ only in the type of mask mandate. Some places mandate N95 and others don't. This is the result:
{kind=link}